
[Ashulia Women and Children Hospital on prevention and protection of children from childhood infections and diseases and reduce postnatal mortality rates.]
December 2022
Prepared by Ashulia Women and Children Hospital
Appropriate infant and young child feeding (IYCF) is critical for growth, and development, and for early prevention of chronic degenerative diseases. Children under two years are at risk of nutritional deficiency and growth retardation due to inadequate breast feeding and poor complementary feeding practices. United Nations Standing Committee on Nutrition estimated that exclusive breast feeding (EBF) for the first six months of life could reduce infant deaths by 13% and adequate nutritious complementary feeding could reduce all under 5 deaths by 6%. Considering the immense importance of IYCF, World Health Organization (WHO) recommendation for IYCF includes exclusive breast feeding of every child below six months of age with initiation of breast feeding within first hour of birth.
Exclusive breastfeeding (EBF) means that the newborn infant is fed only breast milk and no other liquids (not even water) or solids are given, with the exception of oral rehydration salt solution, vitamins, mineral supplements or medicines. Breastfeeding offers tremendous health benefits to both child and mother an effective EBF coverage has been estimated to avert 13%–15% of deaths among children under five years of age especially in middle and low earning settings. Breastfeeding protects the infants against allergies, sickness and obesity; at the same time it reduces the risk of having childhood infections e.g. ear infections and diseases e.g. diabetes and cancer. It decreases postnatal mortality rates. It can help to improve cognitive and motor development and decreases the rates of sudden infant death syndrome. Moreover, breastfed children have been shown to possess higher intelligence quotient (IQ).
In Bangladesh, the trend of practicing EBF among the lactating mothers remained mostly unchanged for a long time. According to the Bangladesh Demographic and Health Surveys (BDHS) report, the prevalence of EBF was nearly 45% in 1993–94 and 1999–2000, 42% in 2004 and 43% in 2007. The prevalence of EBF markedly increased to 64% in the BDHS report in 2011 which further declined to (55%) in the report of BDHS in 2014. The reasons of this rise and fall in EBF prevalence in recent times remain speculative at this point. While the BDHS collects data on national prevalence of EBF, it does not provide detailed information on factors influencing EBF, nor does it present regional rates of EBF and the causes of variation in EBF in between the regions.
A recent study shows that the proportion of exclusively breastfed infant drops sharply from 52% at 2-3 months to 23% at 4-5 months. Understanding the facilitators and barriers driving these patterns is an important first step towards harmful feeding practices. Almost all Bangladesh children are breastfed to some extent in the first year of life, and fortunately continuation of breastfeeding in the second year of life remains common, with 91% continuing to breastfed. And yet Bangladesh has one of the highest rates of malnutrition in South Asia with about half the children less than 5 years of age being underweight or stunted.
Despite the positive effects of breastfeeding, current rates of optimum breastfeeding are low around the world. Among South Asian countries, EBF is highest in Sri Lanka (75.8%) and lowest in Pakistan (37.7%). In Bangladesh, current EBF practices are reported at 55%, which is an increase from 28% in the 1990s. However, EBF trends have fluctuated from year to year, at 42% in 2004, 43% in 2007, 64% in 2011, and 55% in 2014. The median duration of EBF was 2.8 months [11]. In Bangladesh, 17% of children were fed colostrum in the 1990s, increasing to 51% in 2014.
Since 1989, the Bangladesh Breastfeeding Foundation (BBF) has been supporting breastfeeding activities under the primary healthcare system in hospitals and through media. The Government and the BBF contributed to the adjustment of the national code of marketing of breastmilk substitutes in 1993, the introduction of Baby-Friendly Hospital Initiative in 1991, the Maternity Leave Law in 2001, and the policy of optimal duration of EBF for 6 months (180 days) in 2003. In 2011, the Ministry of Health and Family Welfare (MoHFW) prioritized the infant and young child-feeding (IYCF) intervention and have been implementing the IYCF intervention with non-government organizations-NGOs under the leadership of the Institute of Public Health Nutrition (IPHN).
Understanding barriers to breastfeeding is needed to prevent harmful practices. In high income settings, marketing of infant formula and short maternity leave policy are barriers, highlighting the importance of understanding the “market political context.” Understanding the market political context requires investigation and analysis of the entanglement of markets with social and political influences or drivers of behavior. In low income settings, inadequate access to knowledge, delivery outside the health facility, and being psychologically unprepared have been identified as barriers to breastfeeding. In Bangladesh, there are ongoing barriers to breastfeeding despite the implementation of the breastfeeding-promotion program. One study found that the following factors were associated with significantly higher likelihood of initiating breastfeeding within one hour of birth: mothers giving birth in district hospitals, having their visual privacy maintained in the delivery room, newborns crying spontaneously, and newborns being placed in skin-to-skin contact with mothers.
The available broader literature suggests that important barriers to breastfeeding can be identified across
three inter-related domains: individual-level, society-level, and system-level.
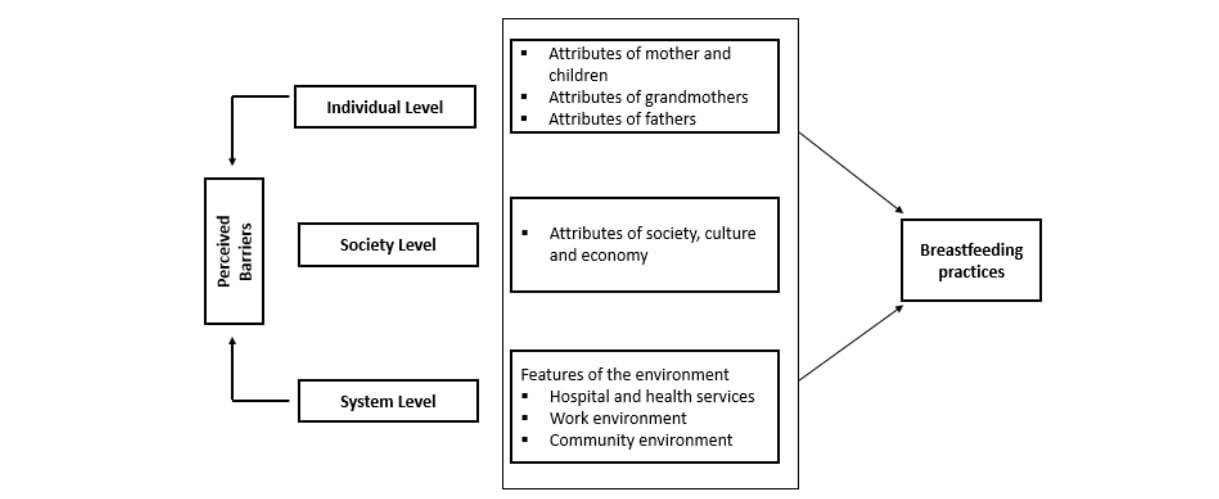
Individual Level Barriers: Barriers at the individual-level are directly related to the attributes of children,
mothers, fathers, grandmothers, and other family members. Examples include:
Misperceptions about breastfeeding: many mothers and grandmothers had misperceptions about feeding colostrum to newborn infants. Many mothers believed that it might cause loose stool as it is very thick and newborn infants are unable to digest it. As a result, these mothers gave honey or sugar-mixed water to their newborn babies. Misperceptions among the mothers also hindered exclusive and continued breastfeeding.
Lack of knowledge and skills among family members and mothers: Mother reported that they did not follow the breastfeeding advice of community health workers (CHWs) because they felt under pressure to follow the instructions of elderly family members to give formula milk or semolina to their children aged less than six months. Adolescent-age mothers sometimes are unaware of proper breastfeeding techniques, resulting in insufficient breastfeeding to their children. This occurred in the case of mothers living with their husbands and having a newborn child in a nuclear family in urban slums.
Society Level Barriers:Sociocultural norms, beliefs, and practices hinder breastfeeding. Examples include:
Mothers are considered a good housewife and admired by other family members if they completed other household chores in time. These expectations put pressure on mothers to dedicate more time to household chores rather than adequately breastfeeding their children.
Feeding formula milk to children was perceived as a symbol of parents’ financial solvency in the community.
Continuation of breastfeeding sometimes are determined by the mother taking into consideration whether her child is male or female. The mothers felt discomfort about continuing to breastfeed their young male children (15–24 months).
Lack of religious knowledge also influenced breastfeeding practices. Some Muslim mothers feel it would be a sin for them if their boy child continues breastfeeding until aged two years old.
System Level Barriers:System-level barriers are those which may influence breastfeeding practices include features of the environment, such as hospital and health services (including resources available, and quality of facilities and of care offered), work environment, and public policy environment.
Adverse effects of cesarean delivery on breastfeeding: Studies suggested that mothers who gave birth through cesarean section made the decision to start formula milk as soon as the deliveries because they claimed to produce insufficient amounts of breast milk. During antenatal care (ANC), these mothers were encouraged by a physician to have a caesarian section in a private hospital or in a clinic in order to have a safe delivery and relief from the pain of normal vaginal delivery.
Attractive media advertisement to initiate breast milk substitutes: Studies suggested that many times mothers are inspired to choose formula milk by attractive media advertisements on televisions that explained the benefits of feeding formula milk and depicted the picture of a healthy child and a smart mother.
Formula milk is advised by physicians: In a recent study a number of mothers reported that they were feeding their children formula milk because physicians and pharmacy shopkeepers willingly prescribed and advised the formula milk when mothers visited them for seeking treatment.
Inadequate facilities and support process in mothers’ work environment: In urban areas,
working mothers are obliged to join the workplace (particularly in garment factories) before their
children are six months old, despite the lack of a daycare center in the workplace to ensure EBF.
A large number of women who work at garment factories in urban Dhaka keep their children in
their rural houses under the care of their paternal or maternal grandmothers. This strategy
enabled working mothers to perform a high volume of work for a good earning without any hassle
of childcare.
Furthermore, sometimes mothers perceive that feeding their children stored breast milk is an
unusual practice, time-consuming, painful, and hassles to them and proxy caregivers. As a result,
proxy caregivers fed formula milk or semolina and often provided low-quality junk food when the
mothers went outside for work.
In the time line from (Jan-Oct), 2022 Ashulia Women & Children Hospital, had 2214 patients’ number that they provided treatments.
The post natal section has 2 divisions – Indoor & Outdoor. Under Indoor & Outdoor section they
have 4 criteria:

Furthermore, the total number of ANC Counselling is 315. Among the children who received
treatment 1036 were boy children and 866 were girl children.
Since, mother’s related informations are vital to track, therefore the age group and how many
mother patients are fall into each groups are described below:
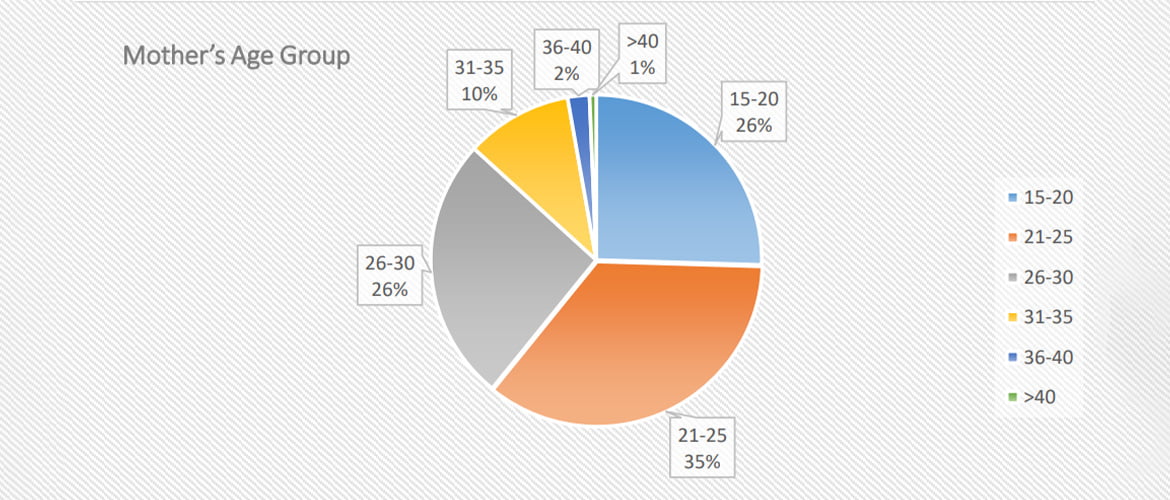
According to the pie chart here we can see that maximum number of mothers are fall into the age group of (21-25) which is 35%. After that the age groups of (15-20) & (26-30) holds 26%. Then in the (31-35) we have 10%. Lastly, the lowest rate of percentage which is 2% and 1% hold by the age group of (36-40) and above 40.
The hospital received complain from the mothers regarding excusive breastfeeding. While
examining the complaints the hospital authority found that not all the complaints are relevant.
Below is the findings of the complaints received from the mothers’.
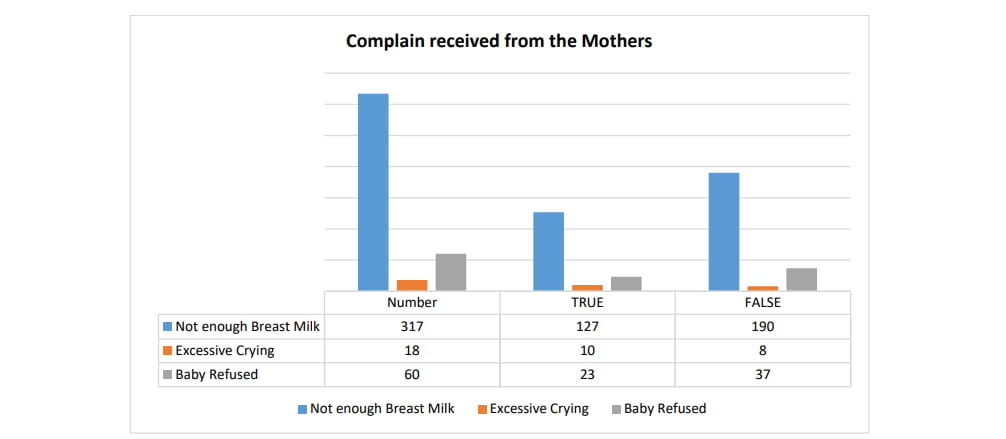
Mothers are facing inconvenience during breastfeeding and there are multiple reasons for that. Ashulia Women & Children Hospital received such feedbacks from the mothers and the total number of that was 2214. But among them only 626 were correct and 1588 were incorrect.
From the correct reasons mostly mothers have trouble to breastfeed because of having short
nipple and the number is 127, which the highest of all. Then because of engorgement (58) as
after giving birth mother’s breast can feel differently with all the changes happing inside the
body. After that the problem occurs because of Inverted nipple (44), Flat nipple (42), and Sore
nipple (29). Lastly, some mothers can also find it difficult due to other reasons as well such as –
Mastitis, Breast abscess or Duct block, also for their adopted child too.
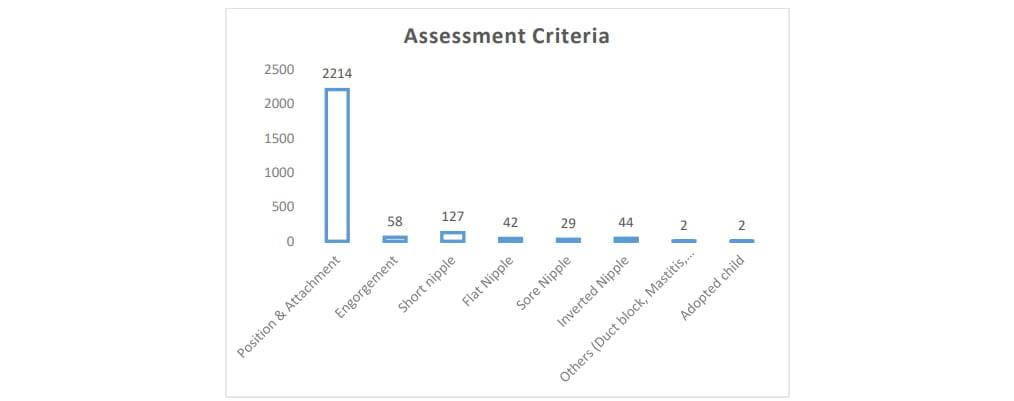
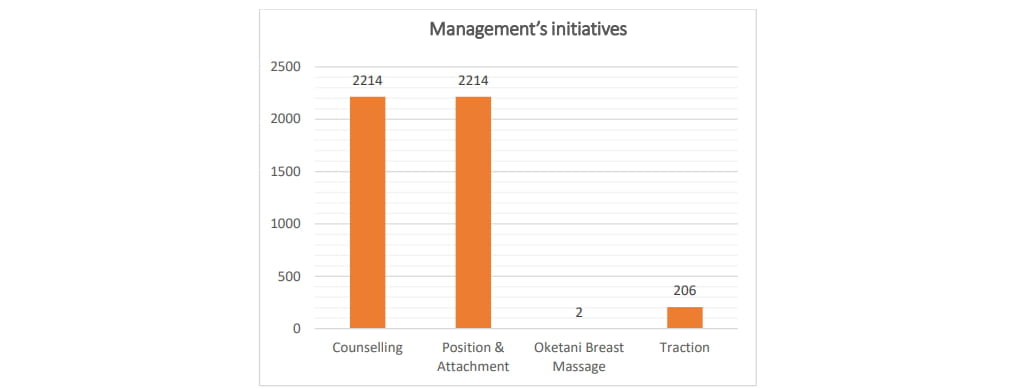
As a responsible hospital the management of the Ashulia Women & Children Hospital under
take some initiatives to help their patients more efficiently. The hospital provided counselling
to total 2214 patients. The number of Position & Attachment is also 2214. For better treatment
they also implies 2 Oketani breast massage which is basically a special types of manual
technique of breast treatment developed by Sotomi Oketani to promote breastfeeding
especially in certain lactation problem like not enough milk or sore nipple or mastitis.
Moreover, they hundled total 206 number of traction.
With an objective to raise awareness among all relevant stakeholders, solving breastfeeding obstacles and motivate the mothers to ensure strong desire of Exclusive Breastfeeding, Ashulia Women and Children Hospital has undertaken a Plan of Action to be implemented.
1. Information Hub Development
